


Triple Negative Breast Cancer (TNBC) With Lung Metastasis Treatment Journey and Case Study
- Nov 1, 2025
- 3 min read
A Malaysian lady at her 55 years old was diagnosed with triple-negative breast cancer (TNBC) in 2024 following imaging that showed a progressively enlarging lesion in the left breast. Histopathology confirmed invasive carcinoma of no special type with medullary pattern, Grade 3, with a Ki-67 proliferation index of approximately 80%, indicating a biologically aggressive tumour subtype.
Immunohistochemistry testing confirmed the tumour was estrogen receptor negative, progesterone receptor negative, and HER2 negative, consistent with triple-negative breast cancer. Genetic analysis also identified BRCA1 and TP53 variants, which are known to be associated with TNBC biology.
She underwent two surgical procedures, including lumpectomy and margin revision. Sentinel lymph node biopsy showed no metastatic involvement (0/3 nodes) at that stage. Following surgery, she underwent a comprehensive oncological treatment regimen including:
6 cycles of chemotherapy
6 cycles of immunotherapy
25 sessions of radiotherapy (March–May 2025)
3 cycles of capecitabine (Xeloda)
Despite aggressive treatment, a PET-CT scan in 2025 revealed disease progression, with findings including:
Newly developed mediastinal and bilateral hilar lymph node metastases
Multiple small lung nodules suspicious for metastatic disease
Persistent post-treatment changes in the left breast region
Multiple FDG-avid mediastinal and hilar lymph nodes, largest measuring 2.0 × 1.2 cm
Several lung nodules, up to 0.6 cm in size
These findings indicated metastatic spread to the lungs and thoracic lymph nodes.
At that point, her oncologist initiated targeted therapy with Olaparib as second line, and at the same time, she also began using ECCT, primarily the ECCT blanket system, as a supportive modality alongside her ongoing oncological care to enhance drug delivery and effect. This approach was undertaken while the patient continued oncologist-directed targeted therapy with Olaparib and regular clinical monitoring.

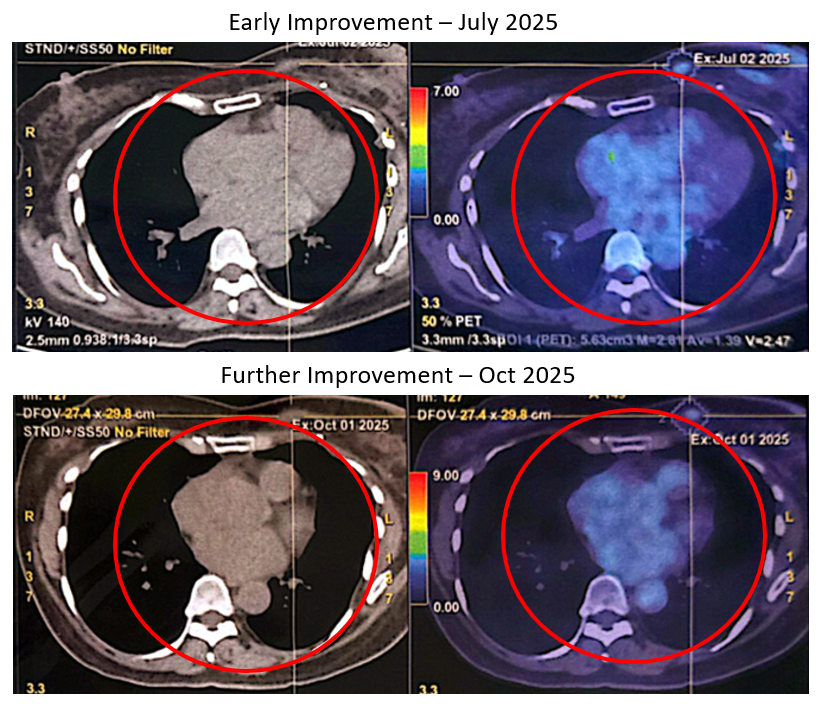
July 2025 PET-CT (Early Improvement)
Approximately six weeks later, repeat imaging showed several encouraging changes:
Mediastinal lymph nodes decreased in both size and metabolic activity
Largest node of 2. 0cm reduced to 1.2 cm
SUVmax dropped from 6.4 to 3.3
Lung nodules decreased in size
Largest nodule reduced from 0.6 cm to 0.5 cm
Metabolic activity in breast skin thickening also decreased
SUVmax reduced from 3.1 to 2.6
These changes suggested partial metabolic and anatomical improvement compared with the previous scan.
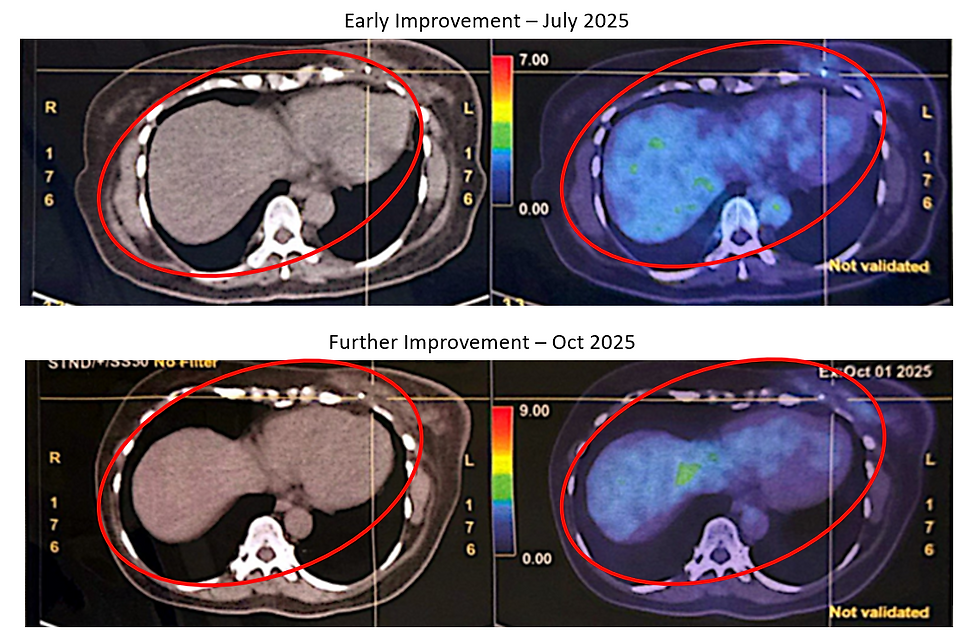
October 2025 PET-CT (Further Resolution)
The subsequent PET-CT scan in October 2025 demonstrated further favourable developments:
Previously FDG-avid mediastinal and hilar lymph nodes had resolved
Most lung nodules had largely resolved, with only very small residual nodules remaining
No new hypermetabolic lesions were identified
The previously noted breast changes remained stable and consistent with post-radiation effects
Importantly, the report concluded:
“No abnormal hypermetabolic foci or metastases elsewhere.”
This represented a marked improvement compared with the metastatic findings seen earlier in May 2025.
Blood Test and Clinical Monitoring
Routine blood tests conducted during follow-up visits showed generally stable results:
Liver and renal function remained within normal limits
Hemoglobin measured around 11 g/dL, slightly reduced but still acceptable
No major biochemical abnormalities were detected
These findings suggested that the patient was tolerating ongoing therapy without major systemic toxicity.
Changes in General Condition
Beyond imaging results, several improvements were noted in the patient’s overall condition:
The patient remained physically active and functional, even continuing to work from home.
Appetite remained good throughout the treatment period.
No significant pain symptoms were reported.
Sleep quality improved somewhat, especially after starting supportive inhalation therapy.
No neurological symptoms such as numbness were reported.
No swelling of the legs or significant mobility limitations were observed.
During review consultations, she appeared well, alert, and able to communicate comfortably, indicating preserved quality of life during ongoing treatment.
Overall Observations
From an observational standpoint, this case illustrates the complexity of treating triple-negative breast cancer, which is known for its aggressive biology and potential for recurrence.
The patient underwent multiple evidence-based treatments including:
Surgery
Chemotherapy
Immunotherapy
Radiotherapy
Targeted therapy (Olaparib)
During the same period, she also incorporated ECCT supportive therapy as part of her treatment strategy.
Over several months of follow-up, imaging demonstrated:
Reduction and eventual resolution of metastatic lymph nodes
Marked reduction of lung nodules
No new metastatic lesions
Stable post-treatment changes in the breast
At the same time, her clinical condition remained stable, with acceptable laboratory parameters and maintained daily function.



Comments